Heavy Menstrual Bleeding on Blood Thinners: What You Need to Know and How to Manage It

Blood Thinner Menstrual Bleeding Risk Calculator
How Your Blood Thinner Affects Your Periods
Different blood thinners carry different risks for heavy menstrual bleeding. Select your medication below to see your risk level and what you can do about it.
Did you know? Studies show about 70% of menstruating women on blood thinners experience heavy periods. This tool helps you understand your specific risk based on your medication.
When you start taking blood thinners-whether it's for a blood clot, atrial fibrillation, or another condition-you’re told to watch for signs of bleeding: bruising, nosebleeds, or cuts that won’t stop. But one of the most common and least discussed side effects? Heavy menstrual bleeding. For women on anticoagulants, periods don’t just get heavier-they can become overwhelming, unpredictable, and life-disrupting. And yet, most doctors don’t ask about it.
Here’s the hard truth: about 70% of menstruating women on blood thinners experience heavy periods. That’s not rare. That’s the norm. And it’s not just about discomfort. It’s about anemia, missing work, constant anxiety, and having to carry emergency changes everywhere. If you’re on a blood thinner and your period has gotten worse since you started, you’re not alone. And there are real, effective ways to manage it-without stopping your medication.
Why Blood Thinners Make Periods Heavier
Blood thinners don’t just prevent clots in your veins and arteries-they affect every part of your body, including your uterus. When you take a drug like rivaroxaban, apixaban, dabigatran, or warfarin, your blood’s ability to clot is lowered. That’s good for preventing strokes and clots. But when your uterine lining sheds during your period, your body needs to form clots to stop the bleeding. With thinners, that process doesn’t work as well.
Normal menstrual bleeding? About 5 to 8 tablespoons of blood over 4 to 7 days. Heavy menstrual bleeding? You’re changing pads or tampons every hour, leaking through, and soaking through clothes. You might be passing clots the size of a golf ball. This isn’t just "a bad period." It’s a medical issue.
Research from the Blood journal in 2022 found that two out of three women who started blood thinners had abnormally heavy bleeding within months. That’s 66.7%. Other studies put the number closer to 70%. Compare that to the general population, where only 10% to 30% of women have heavy periods naturally. Anticoagulants don’t just increase the risk-they multiply it.
Which Blood Thinners Are Worst for Periods?
Not all blood thinners are equal when it comes to menstrual bleeding. Some are much more likely to cause heavy periods than others.
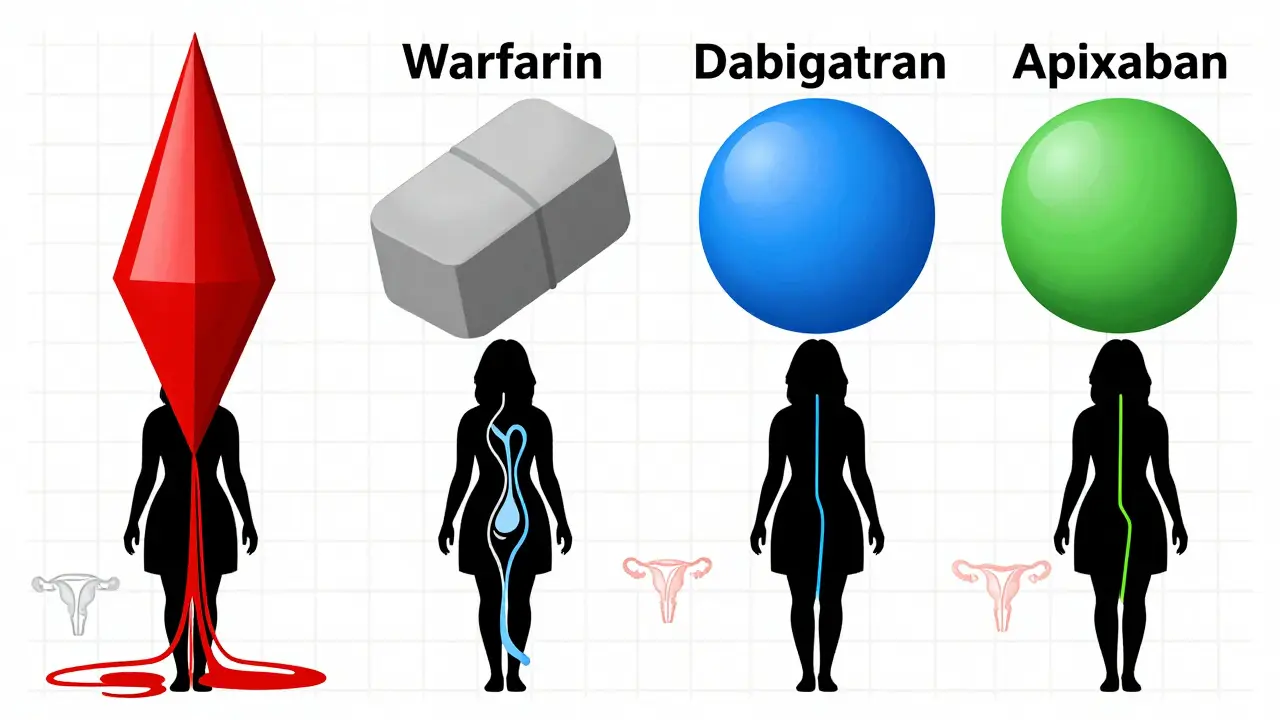
Studies show that rivaroxaban carries the highest risk. Women on rivaroxaban are significantly more likely to report heavy bleeding than those on other drugs. On the other hand, apixaban and dabigatran are associated with lower rates of heavy periods. The difference isn’t just small-it’s meaningful enough that doctors now consider switching anticoagulants as a treatment option.
Warfarin, the older blood thinner, also causes heavy bleeding, but because it requires frequent monitoring and dose adjustments, it’s harder to isolate its effect on periods. Still, if you’re on warfarin and your bleeding has gotten worse, switching to a DOAC (direct oral anticoagulant) like apixaban might help.
Here’s what the data says about risk levels:
| Anticoagulant | Risk Level | Notes |
|---|---|---|
| Rivaroxaban | High | Most associated with heavy bleeding |
| Warfarin | Moderate to High | Variable due to dosing |
| Dabigatran | Low | Lower bleeding risk than rivaroxaban |
| Apixaban | Low | Best profile for minimizing menstrual bleeding |
If you’re on rivaroxaban and struggling with heavy periods, talk to your hematologist about switching. You don’t have to live with it.
What Happens If You Don’t Treat It?
Ignoring heavy bleeding isn’t just inconvenient-it’s dangerous.
First, you can develop iron deficiency anemia. That means fatigue, dizziness, shortness of breath, and brain fog. You might think you’re just tired from work or stress. But if you’re bleeding heavily every month, your body can’t replace the iron fast enough.
Second, you’ll start adjusting your life around your period. Women report carrying extra pads, wearing dark clothes, avoiding travel, skipping work (3-5 days per month, on average), and even avoiding intimacy. One woman on Reddit said she had to leave her daughter’s school play early because she started bleeding through her clothes. Another said she cried in the bathroom at work because she couldn’t find a clean tampon.
And here’s the biggest risk: if you skip doses or stop your blood thinner because you’re scared of bleeding, you’re putting yourself at risk for a life-threatening clot. Studies show that skipping or stopping anticoagulants increases the chance of recurrent blood clots by up to five times. That’s not worth it.
You don’t have to choose between safety and quality of life. There are safe, effective ways to manage the bleeding while staying protected.
Effective Treatment Options (That Won’t Stop Your Blood Thinner)
The good news? You don’t have to stop your anticoagulant. You can treat the bleeding without compromising your protection against clots.
1. Hormonal IUD (Levonorgestrel Intrauterine System)
This is the most effective option for most women. The levonorgestrel IUD (like Mirena or Kyleena) releases a low dose of progesterone directly into the uterus. It thins the uterine lining, reduces bleeding, and in up to 20% of women, stops periods entirely.
Studies show a 70-90% reduction in menstrual blood loss within 3 to 6 months. One woman on r/anticoagulation said: "After getting the Mirena, my periods went from ER visits to nearly nonexistent-while staying on Eliquis. Life-changing."
It’s safe to use with blood thinners. No increased risk of bleeding. No interaction. It lasts 3 to 5 years. And once it’s in place, you don’t have to think about it.
2. Progesterone-Only Pills or Implants
If you don’t want an IUD, progesterone-only pills (like norethisterone) or a subdermal implant (like Nexplanon) are strong alternatives.
The American Society of Hematology recommends a high-dose progesterone regimen: norethisterone 5 mg three times a day for 21 days during your period. This can cut bleeding by 50% or more.
Implants work similarly-they release steady progesterone and reduce bleeding over time. They’re especially good for women who can’t take estrogen.
3. Tranexamic Acid
This is a non-hormonal pill taken only during your period. It works by helping blood clot in the uterus. You take it for 3 to 5 days at the start of your period.
Clinical trials show it reduces bleeding by 30-50%. It’s safe with blood thinners when used correctly. You don’t take it every day-just during bleeding. It’s ideal for women who want to avoid hormones.
4. NSAIDs (Ibuprofen, Naproxen)
Over-the-counter NSAIDs like ibuprofen can reduce menstrual bleeding by 20-40%. They also help with cramps.
But here’s the catch: if you’re already on a blood thinner, adding NSAIDs increases bleeding risk. So talk to your doctor before using them. They might be okay in low doses for short periods, but they’re not a first-line solution.
What About Surgery?
Procedures like endometrial ablation-where the lining of the uterus is burned off-can stop periods in 80-90% of women. But for women on blood thinners, it’s risky.
Because you can’t stop your anticoagulant safely for surgery, the risk of bleeding during or after the procedure is too high. Most doctors avoid it unless absolutely necessary. And even then, you’d need to be bridged with heparin, which adds complexity.
For most women, the IUD or progesterone options are safer, simpler, and just as effective.

Why Your Doctor Might Not Be Talking About This
Here’s the uncomfortable part: most hematologists don’t ask about periods. A 2023 survey by the National Blood Clot Alliance found that 68% of women said their hematologist never asked about menstrual changes after starting blood thinners.
Why? Because it’s not taught. There are no official guidelines yet. The American Society of Hematology and ACOG are working on joint guidelines expected in Q2 2025, but until then, it’s up to you to bring it up.
Don’t wait. If you’re on a blood thinner and your periods are heavier than before, say something. Ask: "Is this normal?" "Can we adjust my medication?" "Can I get an IUD?"
What You Should Do Right Now
If you’re on a blood thinner and your periods are heavy:
- Track your bleeding: How often are you changing? Are you leaking? Are you passing clots?
- Check your iron levels: Get a blood test for ferritin and hemoglobin. Iron deficiency is common and treatable.
- Ask your hematologist: "Is my anticoagulant the one most likely to cause heavy bleeding?" Then ask: "Can we switch to apixaban or dabigatran?"
- Ask your gynecologist: "Can I get a levonorgestrel IUD?" It’s safe, effective, and long-lasting.
- Consider tranexamic acid if you don’t want hormones.
- Don’t skip your blood thinner. The risk of a clot is far greater than the risk of heavy bleeding.
You deserve to feel in control of your body. Heavy periods on blood thinners aren’t normal. They’re a treatable side effect. And you don’t have to suffer through them.
Korn Deno
March 23, 2026 AT 06:19We take drugs to keep us alive and then they wreck the parts of us that make life worth living.
Heavy periods, fatigue, anxiety - it's not a side effect, it's a rewrite of your biology.
You're not broken. Your body's just trying to survive in a system that never asked if you wanted to.
Maybe the real question isn't how to stop the bleeding - but why we accept this as normal.
Why do we treat women's bodies like collateral damage in medical progress?
I don't have answers. Just frustration.
And yeah, I'm on apixaban too. Still bleeding like a faucet.
Aaron Sims
March 24, 2026 AT 17:39Who do you think invented blood thinners? Who profits from the 'solution'? Who writes the studies? Who funds the 'research'? HUH?
Also - why is no one talking about the fact that the FDA approved these drugs WITHOUT mandatory menstrual tracking? That's not an oversight - it's a feature.
They want you bleeding. It creates dependency. It creates more prescriptions. It creates more $$$.
Wake up. This is all a marketing scheme wrapped in medical jargon.
Stephen Alabi
March 25, 2026 AT 16:08It is scientifically inaccurate to assert that '70% of menstruating women on blood thinners experience heavy periods' as if this were a universally quantifiable metric without stratification by age, BMI, parity, or genetic coagulopathy markers.
Furthermore, the recommendation to switch anticoagulants based on observational data from non-randomized cohorts constitutes a gross violation of evidence-based medicine principles.
One must also consider the pharmacokinetic variability of DOACs in relation to CYP3A4 and P-glycoprotein expression - factors entirely omitted in this article.
Additionally, the suggestion to use tranexamic acid without reference to renal clearance thresholds is potentially life-threatening.
I urge all readers to consult a board-certified hematologist before implementing any of these recommendations.
Agbogla Bischof
March 27, 2026 AT 15:48She didn’t even know it was related until she mentioned it to a nurse at a clinic.
They gave her tranexamic acid - no IUD, no switch - just the pill.
It cut her bleeding in half within two cycles.
And yes - she’s still on warfarin.
It’s not rocket science.
Doctors here don’t have fancy guidelines - they just listen.
Ask. Try. Adjust.
You don’t need a PhD to fix this - just a doctor who cares.
Anil Arekar
March 27, 2026 AT 23:17While cardiovascular outcomes are prioritized, reproductive health is treated as secondary - even though it directly impacts quality of life, mental health, and adherence to life-saving therapy.
It is encouraging to see that the American Society of Hematology is developing joint guidelines with ACOG - this represents a necessary convergence of specialties.
However, implementation must be accompanied by mandatory training for clinicians, standardized screening protocols, and patient education materials in multiple languages.
Let us not mistake awareness for equity - systemic change requires institutional commitment, not just Reddit posts.
Elaine Parra
March 28, 2026 AT 11:43My periods are so bad I’ve had to quit two jobs because I couldn’t show up.
My husband says I’m dramatic.
My mom says I should just deal with it.
My doctor says ‘it’s normal’.
Guess what? It’s not normal.
And if you’re not bleeding through your clothes every month, you don’t get to say it’s fine.
Stop gaslighting women.
Stop pretending this isn’t a crisis.
And if you’re a man reading this - shut up and listen.
Kevin Siewe
March 28, 2026 AT 21:54If you're reading this and you're struggling - you're not alone.
It's okay to feel overwhelmed.
It's okay to cry in the bathroom.
It's okay to ask for help.
And it's absolutely okay to advocate for yourself - even if your doctor seems dismissive.
You deserve to live without fear of leaking through your jeans.
One step at a time.
You’ve got this.
James Moreau
March 29, 2026 AT 07:10It's rare to see a medical topic handled with both scientific rigor and human empathy.
Most articles either drown you in jargon or oversimplify to the point of being useless.
This strikes the right balance.
Especially the part about not stopping your blood thinner - that’s critical.
Thanks for putting this out there.
J. Murphy
March 30, 2026 AT 14:23how do they even test this??
did they just ask women to rate their bleedings on a scale of 1-10??
also who even uses tranexamic acid??
that sounds like something from a 90s russian clinic
Seth Eugenne
March 30, 2026 AT 17:01My periods went from "I need a change every hour" to "I barely notice it".
And I didn’t even have to think about it after the first week.
Best decision I’ve ever made.
Also - my anxiety dropped like a rock.
Not because of hormones - because I stopped being scared every time I left the house.
Thank you for writing this.
💙
rebecca klady
April 1, 2026 AT 03:03Thank you.
Namrata Goyal
April 1, 2026 AT 17:00In India, women have been dealing with heavy bleeding for centuries - no IUDs, no DOACs, no tranexamic acid.
We use neem, ashoka bark, and turmeric paste.
And we don’t cry about it.
Maybe the problem isn’t the blood thinner - it’s that modern women have lost touch with their bodies.
Just saying.