Look-Alike, Sound-Alike Medication Names: How to Spot and Prevent Errors

Imagine you are in a busy hospital ward. The lights are dim, the phones are ringing, and you have just received a verbal order for "hydrocodone." You grab a vial that looks exactly right. It is only when you double-check the label seconds later that you realize it says "hydromorphone." That tiny difference in spelling could mean the difference between pain relief and respiratory failure.
This isn't a hypothetical nightmare; it is a documented reality in healthcare systems worldwide. These mistakes stem from Look-Alike, Sound-Alike (LASA) medications, which are drugs with similar names, packaging, or physical appearances that lead to dangerous dispensing and administration errors. According to data from the Anesthesia Patient Safety Foundation, LASA errors account for up to 25% of all medication errors. In some studies, drug name confusion alone makes up nearly two-thirds of these incidents. This article breaks down why these errors happen, the specific drugs involved, and the practical strategies healthcare providers use to prevent them.
Why Do LASA Errors Happen?
You might think that with electronic health records and barcode scanners, these errors would be a thing of the past. But human factors still play a massive role. LASA errors occur through four main mechanisms: orthographic (visual similarity of text), phonetic (sound-alike names), packaging (similar box design), and physical appearance (pill shape and color).
A landmark study published in Medical Care developed a model using 22 computerized measures to assess drug-name confusion risks. The results were clear: every measure of similarity proved to be a significant risk factor for error. The higher the similarity score between two drug names, the higher the odds of a mistake. This creates a "significant increasing trend" in error rates as names become more alike.
Context matters too. A 2022 study in Pharmacy Practice found that anticipatory errors often spike during busy periods or shift changes. When pharmacists and nurses are under pressure, crucial details like drug strengths can be overlooked. For example, simvastatin 10 mg and simvastatin 20 mg were identified as the most frequent LASA pair in hospital databases. Even though they are the same drug, the slight difference in strength leads to dosing errors that can cause muscle damage or liver issues.
The Most Dangerous Drug Pairs
Not all look-alike drugs carry the same level of risk. The Institute for Safe Medication Practices (ISMP) categorizes LASA pairs into critical risk levels. Some combinations involve high-alert medications, where a small error can lead to death or serious harm.
| Drug Pair | Category | Risk Factor |
|---|---|---|
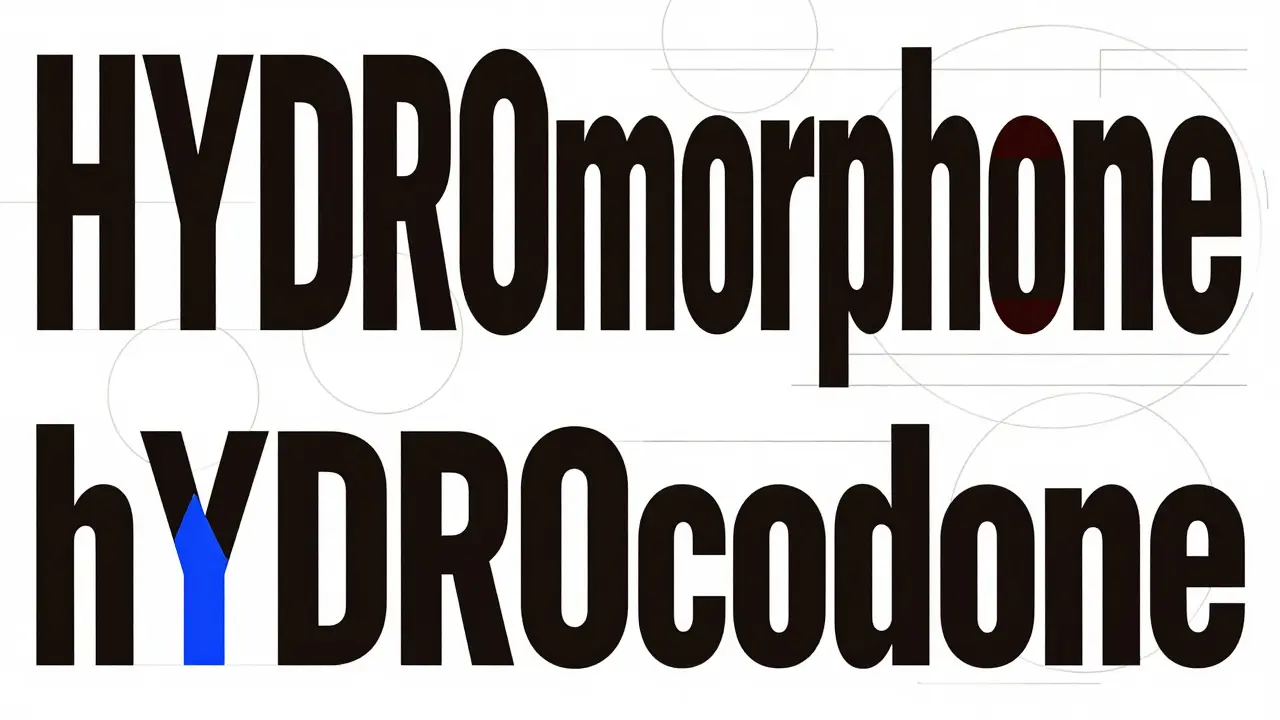
| HYDROmorphone / hYDROcodone | Opioids | Respiratory depression, overdose |
| cisPLATIN / caraPLATIN | Chemotherapy | Toxicity, ineffective cancer treatment |
| levoTHYROXINE / SYNTHROID | Thyroid Hormones | Metabolic imbalance, cardiac stress |
| vecurONIUM / midazoLAM | Anesthetics | Paralysis vs. sedation confusion |
| naltrexone / naloxone | Opioid Antagonists | Addiction treatment vs. emergency reversal |
Notice the capitalization in the first two pairs? That is not random. It is a deliberate safety strategy called Tall Man Lettering, which we will discuss next. The FDA MAUDE database reports at least 128 deaths attributed to LASA errors between 2018 and 2022, highlighting the lethal potential of these confusions, especially with chemotherapy agents like doxorubicin and daunorubicin.
Tall Man Lettering: Does It Work?
Tall Man Lettering (TML) is a visual aid technique where certain letters in drug names are capitalized to highlight differences between similar-sounding or looking names. The FDA has implemented this for over 200 medication pairs since 2001. You see it everywhere now: DOXEpacin vs. doxycycline, or CLOPiDogrel vs. cloZApiDe.
The idea is simple: by breaking the visual pattern of the word, your brain is forced to slow down and notice the difference. However, its effectiveness is debated. A systematic review in the Journal of Pharmacy Practice and Pharmaceutical Sciences concluded that TML is "marginally effective" and may create a "quasi-placebo effect." This means it helps if staff are aware of its purpose, but it doesn't automatically prevent errors on its own.
For TML to work, it needs to be part of a broader system. It should appear on labels, in electronic health records (EHRs), and on pharmacy shelves. If it is only on one surface, the cognitive load remains high. Dr. Michael Cohen, President of ISMP, testified before the FDA that while safeguards help, the best prevention is stopping confusing names from entering the market in the first place.
Technology and Systemic Solutions
Human vigilance is essential, but it is not enough. Technology plays a huge role in intercepting LASA errors before they reach the patient. Electronic prescribing systems now include clinical decision support (CDS) tools that flag potential LASA confusions. For instance, Epic’s "SafeMed" module reduced name-confusion errors by 28.7% in a 12-hospital study.
However, technology introduces new challenges. Alert fatigue is real. If a system flags every minor similarity, clinicians start ignoring the warnings. This is why customization is key. The Joint Commission recommends that hospitals maintain their own personalized LASA lists based on their specific formulary, rather than using generic external lists. These lists should be reviewed and updated annually.
Barcode medication administration (BCMA) is another critical layer. Scanning the patient’s wristband and the medication barcode ensures that the right drug goes to the right person at the right time. Yet, BCMA systems can fail if the barcode on the package is incorrect or if staff bypass the scan due to workflow pressures. A 2023 analysis by Merative showed that healthcare systems implementing comprehensive LASA protocols-including both tech and process changes-reduced related errors by 37.4% on average.

What Can Healthcare Providers Do?
If you work in healthcare, you are on the front lines of LASA prevention. Here are actionable steps to reduce risk:
- Personalize Your LASA List: Work with your pharmacy team to identify the top 10-20 LASA pairs relevant to your unit. Post these prominently in medication rooms.
- Use Full Generic Names: Avoid abbreviations. Say "metoprolol succinate" instead of "toprol XL" or "meto." Ambiguity breeds error.
- Verify Verbal Orders: Repeat back the entire order, including dose, route, and frequency. Ask for clarification if any part sounds similar to another common drug.
- Check Packaging Visually: Don’t rely solely on memory. Compare the box and bottle to the previous supply. Note differences in color, shape, and labeling.
- Report Near-Misses: If you catch an error before it reaches the patient, report it. This data helps institutions identify systemic weaknesses and update their LASA lists.
Training is also vital. The American Society of Health-System Pharmacists (ASHP) recommends 2-4 hours of annual education for clinical staff, with additional quarterly refreshers for high-risk departments like oncology and critical care. Simulation training can be particularly effective, allowing staff to practice recognizing LASA pairs in low-stakes environments.
The Future of LASA Prevention
The landscape of medication safety is evolving. The FDA’s 2023 draft guidance proposes mandatory orthographic and phonetic testing for all new drug names using standardized algorithms. This aims to prevent confusing names from being approved in the first place. In 2022, the FDA denied 34 new drug name applications specifically due to LASA concerns, up from 22 in 2018.
Innovations are also emerging. The Agency for Healthcare Research and Quality (AHRQ) is funding a study at Johns Hopkins testing AI-powered voice recognition systems. These systems aim to detect potential LASA confusions during verbal medication orders, with preliminary results showing 89.3% accuracy in identifying high-risk pairs.
Long-term, experts like Dr. Donald Berwick believe that a systematic approach combining regulatory oversight, technological solutions, and human-centered design could reduce LASA incidence by 80% within a decade. However, resource-constrained settings still face significant challenges. Enterprise adoption of comprehensive LASA protocols stands at 72% in large U.S. hospitals but only 38% in smaller facilities.
Until then, awareness remains our strongest tool. By understanding how LASA errors occur and actively engaging in prevention strategies, healthcare providers can protect patients from these hidden dangers.
What are the most common look-alike, sound-alike drug pairs?
Some of the most frequently confused pairs include hydrocodone/hydromorphone, levothyroxine/synthroid, vecuronium/versed, and cisplatin/carboplatin. These pairs are often highlighted in institutional LASA lists due to their high risk of causing severe adverse events.
How does Tall Man Lettering help prevent medication errors?
Tall Man Lettering uses capitalization to emphasize differences between similar drug names (e.g., DOXEpacin vs. doxycycline). This visual cue forces the reader to slow down and notice the distinction, reducing the likelihood of misreading the label.
Who is most at risk for LASA medication errors?
Patients receiving high-alert medications such as opioids, insulin, anticoagulants, and chemotherapy agents are at highest risk. Additionally, errors are more likely during busy shifts, handoffs, or when staff are fatigued.
Can technology completely eliminate LASA errors?
No technology can completely eliminate human error. While EHR alerts and barcode scanning significantly reduce risks, they require proper implementation and user compliance. Alert fatigue and system bypasses remain challenges.
What should I do if I suspect a LASA error has occurred?
If you suspect an error, stop administration immediately, assess the patient for adverse effects, and notify the prescribing provider and pharmacist. Document the incident and report it through your institution’s near-miss or error reporting system to help prevent future occurrences.