Variceal Bleeding: How Banding, Beta-Blockers, and Prevention Save Lives
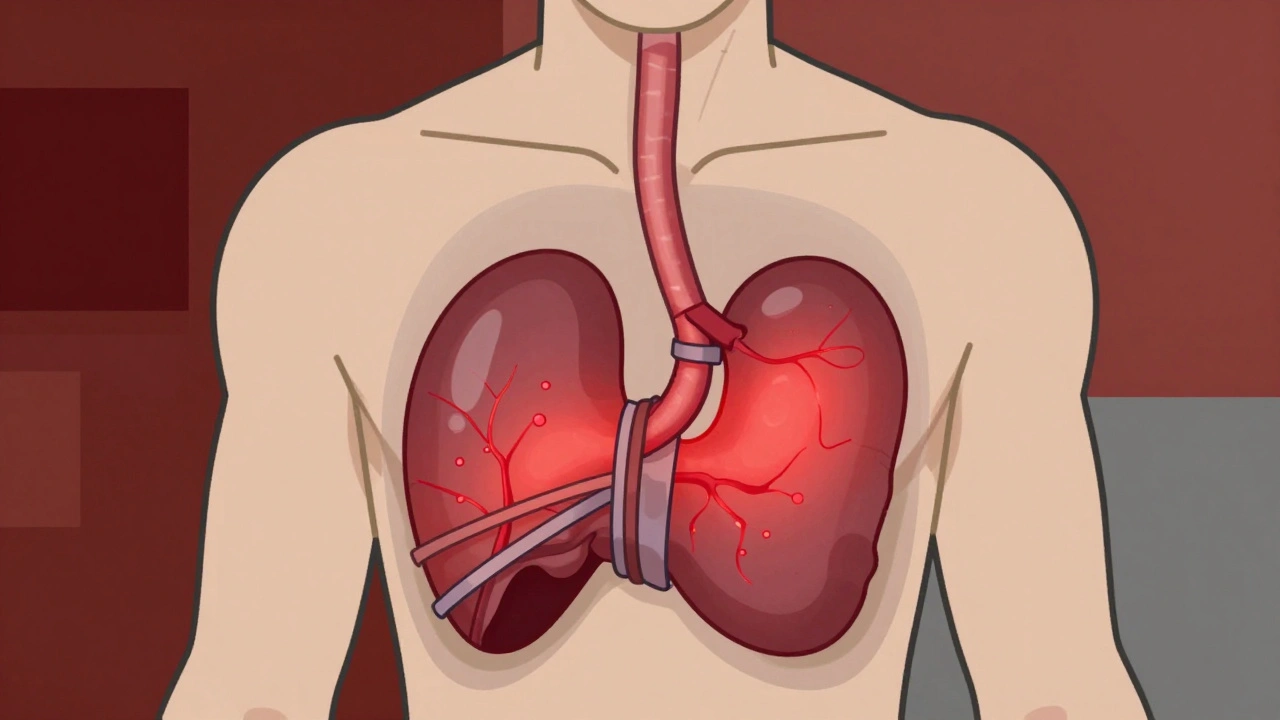
When your liver is damaged by cirrhosis, pressure builds up in the portal vein - the main blood vessel carrying blood from your intestines to your liver. Over time, this pressure forces blood to find new paths, creating swollen, fragile veins in your esophagus or stomach. These are called varices. And when they burst, it’s not just a medical emergency - it’s a fight for your life. About 1 in 5 people who bleed from varices die within six weeks. But here’s the good news: we know how to stop it. And we’ve got three powerful tools: endoscopic banding, beta-blockers, and smart prevention.
What Happens When Varices Bleed?
Variceal bleeding doesn’t sneak up. It hits hard. You might vomit bright red blood, pass black, tarry stools, or feel dizzy and faint. The veins are thin-walled and under high pressure - like a balloon stretched too far. Once they rupture, bleeding can be massive and fast. The key is acting within hours, not days.
Most cases happen because of long-term liver damage from alcohol, hepatitis B or C, or fatty liver disease. The liver scars, blocks blood flow, and pressure backs up. When portal pressure hits 12 mmHg or more, bleeding risk spikes. That’s why people with advanced cirrhosis need regular monitoring - even if they feel fine.
Endoscopic Banding: The Gold Standard for Stopping Bleeding
If you’re actively bleeding, the fastest, most reliable way to stop it is endoscopic band ligation (EBL). This isn’t surgery. It’s done through an endoscope - a thin tube with a camera - passed down your throat. The doctor uses a special device to place tiny rubber bands around each varix. The bands cut off blood flow, the vein shrinks, and scar tissue forms. Within minutes, the bleeding slows. In 90-95% of cases, it stops completely.
Timing matters. Guidelines say banding must happen within 12 hours of admission. Delays increase death risk. High-volume centers - those doing over 50 banding procedures a year - have 15% lower rebleeding rates than low-volume ones. That’s because experience matters. A skilled endoscopist can see and treat even tricky cases where blood makes visualization hard.
Most patients need 3 to 4 sessions, spaced 1 to 2 weeks apart, to fully eliminate the varices. Each session costs between $1,200 and $1,800 in the U.S. Some people report throat pain for weeks after. Others say they were discharged in 3 days with no issues. The technology has improved too. New multi-band devices like the Boston Scientific Six-Shot system cut procedure time by 35% compared to older single-band tools.
But banding isn’t perfect. It doesn’t work as well for varices in the stomach. For those, a different procedure called BRTO (balloon-occluded retrograde transvenous obliteration) has better outcomes. And if bleeding keeps coming back, or if your liver is very damaged, you might need a TIPS - a shunt placed inside the liver to redirect blood flow. But TIPS comes with risks: up to 30% of patients develop brain fog from hepatic encephalopathy.

Beta-Blockers: The Silent Shield Against Rebleeding
Stopping the first bleed is critical. Stopping the next one is even more important. About half of people who survive a variceal bleed will bleed again within a year - unless they’re on beta-blockers.
Non-selective beta-blockers (NSBBs) like propranolol and carvedilol reduce pressure in the portal vein by slowing your heart and relaxing blood vessels in the gut. The goal? Lower your hepatic venous pressure gradient (HVPG) to 12 mmHg or below, or cut it by 20% from baseline. That’s the sweet spot where rebleeding risk drops by half.
Carvedilol is now preferred over propranolol in many cases. In a 2021 trial, it lowered portal pressure by 22% compared to 15% with propranolol. And both cut rebleeding risk by about 50% compared to no treatment. Propranolol costs $4-$10 a month as a generic. Carvedilol? Around $25-$40. But for many, the better results justify the price.
Side effects are real. Fatigue, dizziness, low heart rate - these make some people quit. One patient on Reddit said propranolol left him too tired to get out of bed. He switched to carvedilol and felt better. But about 25-30% of patients can’t tolerate therapeutic doses. That’s why doctors start low and go slow. You don’t want your blood pressure to crash.
Important: Beta-blockers alone won’t stop active bleeding. They’re for prevention - before or after a bleed. The 2022 AASLD guidelines say they should never be used alone during an active bleed. You need banding first. Then beta-blockers to keep you safe long-term.
Prevention: Catching Varices Before They Burst
The best way to avoid a bleed is to find varices early. If you have cirrhosis, you should get an endoscopy every 1-2 years. If small varices are found, you might start beta-blockers even if you’ve never bled. That’s called primary prevention.
Carvedilol is now being studied as a possible first-line option for primary prevention - even instead of banding - in high-risk patients. A 2023 study in the New England Journal of Medicine showed carvedilol was just as good as banding at preventing first bleeds. That could change practice. Banding is invasive. Beta-blockers are pills. If carvedilol can do the job safely, why not?
But prevention isn’t just drugs. It’s also about protecting your liver. Stop drinking. Get vaccinated for hepatitis A and B. Manage your weight. Avoid NSAIDs like ibuprofen - they can worsen bleeding risk. And if you’re on beta-blockers, never stop them suddenly. That can trigger a rebound spike in pressure - and a bleed.
What Doesn’t Work - And What’s Coming Next
Sclerotherapy - injecting chemicals to harden varices - used to be common. But it’s outdated now. Banding is safer and more effective. Sclerotherapy causes more strictures (narrowing) and rebleeding.
Terlipressin and octreotide are vasoactive drugs used in the ER to buy time before banding. They help reduce bleeding, but they don’t replace endoscopy. A new long-acting version of octreotide (Sandostatin LAR) now lets patients get one monthly shot instead of daily injections. That could help with adherence - right now, only 62% of people stick with daily doses.
Looking ahead, AI might predict who’s about to bleed by analyzing scans and lab values. The PORTAS trial is testing a new way to place TIPS shunts that could make the procedure available in 75% of U.S. hospitals instead of just 45%. And researchers are exploring drugs that directly reduce liver scarring - which could stop varices from forming in the first place.
Living With the Risk
Surviving a variceal bleed changes your life. You’ll need frequent follow-ups. You’ll take meds every day. You’ll dread the next endoscopy. One patient on HealthUnlocked said, "I dread the banding appointments every 2 weeks, but I know it’s saving my life."
But here’s the truth: with the right care, you can live years - even decades - after a bleed. The key is sticking with the plan. Banding when needed. Taking your beta-blockers. Avoiding alcohol. Seeing your doctor regularly. And knowing that even though the risk never fully disappears, you’re not powerless.
There’s no magic cure yet. But we’ve got the tools. And if you use them right, you’re far more likely to outlive the bleeding than to die from it.
Can variceal bleeding be prevented without surgery?
Yes. For people with cirrhosis who have small varices but haven’t bled yet, non-selective beta-blockers like carvedilol or propranolol can reduce the risk of a first bleed by about 50%. Regular endoscopy helps catch varices early. Avoiding alcohol and managing liver health are also critical. Surgery or banding is only needed if varices are large or if bleeding has already happened.
Is endoscopic banding painful?
The procedure itself is done under sedation, so you won’t feel anything. Afterward, some people have sore throat, chest discomfort, or mild pain when swallowing for up to two weeks. This is normal and usually improves on its own. Severe pain or trouble swallowing could signal a complication like an ulcer or stricture, and should be checked right away.
Why is carvedilol better than propranolol for varices?
Carvedilol reduces portal pressure more effectively than propranolol - about 22% versus 15% - because it also blocks alpha receptors, which helps relax blood vessels in the liver. Studies show it’s just as good at preventing rebleeding, and in some cases, better at preventing first bleeds. It’s now recommended as a first-choice beta-blocker for both primary and secondary prevention, especially when patients can tolerate it.
Can I stop taking beta-blockers if I feel fine?
No. Stopping beta-blockers suddenly can cause a dangerous rebound increase in portal pressure, which may trigger a life-threatening bleed. Even if you feel well, your varices are still there. Always talk to your doctor before making any changes. If side effects are a problem, your doctor can adjust the dose or switch you to a different medication.
How often do I need endoscopic banding?
After a bleed, you’ll typically need 3 to 4 banding sessions, spaced 1 to 2 weeks apart, to completely remove the varices. After that, you’ll need follow-up endoscopies every 6 to 12 months to check for new varices. If you’re on beta-blockers and have no varices left, you might only need endoscopy every 2 years. Your doctor will tailor the schedule based on your liver health and risk level.
What happens if banding doesn’t stop the bleeding?
If banding fails - which happens in about 10-15% of active bleeding cases - doctors will use vasoactive drugs like terlipressin or octreotide to stabilize you. Then they’ll consider TIPS (a shunt placed inside the liver) or, in rare cases, emergency surgery. TIPS is very effective for high-risk patients but carries a risk of brain fog. The choice depends on your liver function, how fast you can get the procedure, and your doctor’s expertise.
Are there alternatives to beta-blockers for preventing variceal bleeding?
For primary prevention, beta-blockers are still the standard. But for patients who can’t take them, endoscopic banding can be used even before a bleed occurs - especially if varices are large. There’s also emerging research on drugs that reduce liver scarring, but these aren’t widely available yet. For now, if you can’t tolerate beta-blockers, banding is the next best option.
How do I know if I’m at risk for variceal bleeding?
If you have cirrhosis, you’re at risk. Other signs include enlarged spleen, fluid in the belly (ascites), or jaundice. Your doctor will order an endoscopy to check for varices. If you’ve had a previous bleed, your risk is much higher. Regular monitoring and avoiding alcohol are your best defenses.
Tommy Walton
December 2, 2025 AT 03:33Louise Girvan
December 3, 2025 AT 10:13Michelle Smyth
December 3, 2025 AT 21:19And yet, here we are, banding veins like garden hoses, while the ontological rupture of hepatic fibrosis remains unaddressed. Carvedilol’s alpha-blockade? A Band-Aid on a hemorrhaging soul.
Patrick Smyth
December 4, 2025 AT 01:55patrick sui
December 6, 2025 AT 00:44Also-anyone else think AI-driven risk prediction is the next frontier? Imagine an algorithm that flags your next bleed 72hrs before it happens. That’s sci-fi becoming real.
Declan O Reilly
December 7, 2025 AT 04:26Conor Forde
December 8, 2025 AT 01:30Meanwhile, the real solution-detoxing your liver with turmeric, celery juice, and cold plunges-is buried under $1800 bills and FDA-approved placebo rituals. I’ve been doing this for 3 years. My liver enzymes? Normal. My docs? Furious.
James Steele
December 8, 2025 AT 06:43soorya Raju
December 9, 2025 AT 06:35Grant Hurley
December 10, 2025 AT 17:35Still scared every time I go for an endo. But I’m alive. And I’m not gonna waste it. Thanks for the real talk.
Shannon Gabrielle
December 12, 2025 AT 16:28ANN JACOBS
December 14, 2025 AT 09:40It is not perfect. It is not glamorous. But it is *proven*.
Patients who adhere to surveillance, medication, and lifestyle changes often live for decades. This is not a death sentence-it is a call to disciplined living. Please, for the love of all that is holy, do not stop your beta-blockers. Do not underestimate the power of the simple things.
Nnaemeka Kingsley
December 14, 2025 AT 10:09